Post-traumatic stress disorder (PTSD) is a highly debilitating condition that can significantly impact an individual’s wellbeing, productivity at work, professional and personal relationships, and quality of life in general [1, 2].
PTSD can be diagnosed after specific symptoms are exhibited for more than 6 months following the exposure to one or more emotionally challenging events [3]. PTSD symptoms may include:
• Nightmares
• Flashbacks
• Intrusive thoughts
• Increased alertness (hypervigilance)
• Reduced ability to focus
• Poor sleep
• An altered sense of self and/or reality
In the United States, it has been estimated that approximately 7% of the adult population exhibit PTSD symptoms [4], with a high incidence among military veterans and public health care workers [5-8]. The high number of cases among would population and the severe effects of PTSD on the individual’s quality of life have been the object of accumulating research in the attempt of devising effective interventions.
Currently, prolonged exposure therapy (PET) is the intervention with the strongest scientific support [9]. However, response to PET can be limited in some individuals, which has raised concerns about its applicability in complex cases, including those of multiple and repeated childhood abuse at very early stages of life [10].
In these cases, clinical progress is more likely to be made if neurophysiological dysregulation is tackled using more targeted, reliable, and objective methods. In this context, Neurofeedback has shown promise in alleviating the physiological symptoms associated with PTSD [11, 12], as a stand-alone or complementary treatment.
Patients with emotional disturbances treated with Neurofeedback show improvements in the ability to cope with difficult emotions and can learn to respond appropriately to emotionally challenging situations [13]. Several studies have also demonstrated the effectiveness of Neurofeedback in the treatment of chronic PTSD when other interventions produce little or no change.
For example, in a 2016 case study carried at the University of Amherst, Massachusetts, Fisher, and colleagues demonstrated that after treatment with Neurofeedback in combination with psychotherapy, a woman with severe developmental trauma and with PTSD symptoms that were deemed “untreatable” significantly improved her ability to regulate emotions and to engage in/benefit from psychotherapy [14].
Another study with two PTSD patients with torture and refugee experiences who displayed treatment-resistant PTSD found that adding personalized neurofeedback treatment to their existing therapeutic regimes, produced clinically significant decreases in symptoms [15].
Moreover, both participants showed improvements in cognitive functions, including attention and memory. The authors of the study suggested that Neurofeedback helped the patients to “unblock” by lowering the high level of physiological arousal or affect instability. As a result of becoming better regulated and less aroused, they also become more receptive to other therapeutic interventions.
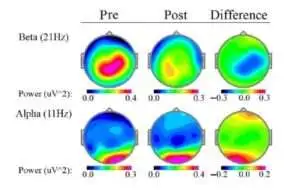
Fig.1 shows the effects of 26 sessions of neurofeedback delivered over a period of 8 weeks on a 50-year-old male with chronic PTSD, dysthymia (chronic depression accompanied by chronic irritability), and panic disorder. As a child, he had been the victim of physical and psychological abuse and, after a year of cognitive behavioral therapy (CBT), he still suffered from insomnia, low control of mood swings or anger, was severely depressed, and had daily panic attacks.
At the time of his referral, he was medicated with alprazolam 1mg/day, venlafaxine 75mg/day, and Valeriana at night. He also had hypertension, which was medicated with candesartan 16mg/day for hypertension.
The electroencephalogram (EEG) taken before treatment revealed over arousal as suggested by low-voltage fast waveforms with excessive widespread beta activity and disorganized fast posterior alpha rhythm.
During his neurofeedback treatment, the arousal gradually decreased, and the patient started to more fully engage in trauma therapy. He started dealing with some of his most distressing traumatic memories and incorporating self-regulation techniques (e.g., breathing) into his daily routines. As affect became more efficiently regulated, it was possible for the therapist to start working on the patient’s relationship with his family and with his past.
On completion of the full neurofeedback treatment, the patient was no longer having panic attacks, his sleep became normal and his irritability disappeared. Importantly, by the end of treatment, all his psychotropic medication was discontinued and he remained only on candesartan for hypertension.
Conclusion
Neurofeedback is an effective treatment for PTSD, and in particular for drug-resistant symptoms of abnormal emotion regulation. It can be used as a standalone intervention or in combination with pharmacotherapy and/or trauma therapy.
References
- Chopra, M.P., et al., PTSD is a chronic, fluctuating disorder affecting the mental quality of life in older adults. Am J Geriatr Psychiatry, 2014. 22(1): p. 86-97.
- Pagotto, L.F., et al., The impact of posttraumatic symptoms and comorbid mental disorders on the health-related quality of life in treatment-seeking PTSD patients. Compr Psychiatry, 2015. 58: p. 68-73.
- Association, A.P., Diagnostic and Statistical Manual of Mental Disorders. 5th ed. ed. 2013, Washington, DC: American Psychiatric Association
- Kessler, R.C., et al., Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry, 2005. 62(6): p. 593-602.
- Kulka, R.A., Schlenger, W. A., Fairbanks, J. A., Hough, R. L., Jordan, B. K., Marmar, C. R., Cranston, A. S., Daniel S. W., Grady D. A. , Trauma and the Vietnam War generation: Report of findings from the National Vietnam Veterans Readjustment Study. 1990, New York, NY: Brunner/Mazel
- Kang, H.K., et al., Post-traumatic stress disorder and chronic fatigue syndrome-like illness among Gulf War veterans: a population-based survey of 30,000 veterans. Am J Epidemiol, 2003. 157(2): p. 141-8.
- McAlonan, G.M., et al., Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Can J Psychiatry, 2007. 52(4): p. 241-7.
- Luftman, K., et al., PTSD in those who care for the injured. Injury, 2017. 48(2): p. 293-296.
- Difede, J., M. Olden, and J. Cukor, Evidence-based treatment of post-traumatic stress disorder. Annu Rev Med, 2014. 65: p. 319-32.
- van der Kolk, B.A., The body keeps the score: Brain, mind, and body in the healing of trauma. 2015, New York, NY: Penguin Viking.
- Kadosh, K.C., Zich, C., Lisk, S., & Lau, J., Using Functional-Connectivity Neurofeedback to Change Emotion Regulation Networks in Pre-Clinically Anxious Adolescents. Biological Psychiatry, 2017. 81.
- Keynan, J., Hendler, T., Amygdala-neurofeedback reduces traumatic stress vulnerability. Biological Psychiatry,, 2017. 81.
- Rolston, A., & Lloyd-Richardson, E. , What is emotional regulation and how do we respond to it? n.d., Ithaca, NY: Cornell Research Program for Self-Injury Recovery
- S.F., F., Neurofeedback ffect regulation and attachment: a case study and analysis of anti-social personality. International Journal of Behavioral Consultation and Therapy, 2007. 3.
- Askovic, M., et al., Neurofeedback as an adjunct therapy for treatment of chronic posttraumatic stress disorder related to refugee trauma and torture experiences: two case studies. Australas Psychiatry, 2017. 25(4): p. 358-363.