Impulsivity is generally described as the tendency of an individual to act and behave with little or no forethought, hardly considering the consequences a given behavior might have on the self or on the community [1].
Clinical research shows that impulsive behaviour is a risk factor for substance abuse [1-5] and studies demonstrate that it is associated with poor clinical outcomes [6, 7] and relapse, even after long withdrawal periods [8, 9].
Impulsivity is usually assessed through clinical interviews and self-reported questionnaires [10, 11] which mainly measure three different components:
- Attentional impulsivity (tendency to make quick decisions and poor ability to focus on specific tasks)
- Motor impulsivity (the tendency to act without thinking)
- Non-planning impulsivity (the reduced ability or interest to plan ahead and consider the future
While impulsive decision making and impulsive behavior appear to be heavily based on the cognitive/attentive domain [11-13] increased physiological arousal and a wide range of emotional states such as anxiety, anger, sadness, or joy are also associated with impulsivity [14, 15].
From a neurobiological point of view, higher depressive symptoms and impulsivity are associated with both structural and functional anomalies in the brain, including the prefrontal cortex [16-20] and, as these anomalies reflect changes in the electroencephalogram (EEG) [21-24], EEG-based therapeutic interventions for addiction have been explored in research studies.
One of these interventions is EEG-neurofeedback training, is a learning-based form of biofeedback aimed at facilitating self-regulation of EEG activity in target brain regions and networks [25, 26]. EEG-neurofeedback training has been shown to be useful in the treatment of drug addiction, reducing impulsivity and increasing abstinence rates [27], also playing a role at lowering reactivity to drug-related stimuli [28].
Other neurofeedback research [29] also indicates that neurofeedback not only contributed to modulate impulsivity in long-term abstinent addicts but also reduced anxiety and depression symptoms, hence lowering the likelihood for relapse [30-32].
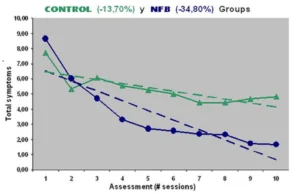
Fig.1 Clinical progression during neurofeedback therapy (the average of clinical symptoms for all subjects/each session is shown over the whole treatment period. NFB: neurofeedback).
Conclusions
Research indicates that neurofeedback training effectively modulates impulsivity in long-term abstinent individuals with history of drug addiction, and that improved control of impulsivity prevents relapse, not only in substance abuse but also in violent behavior.
Moreover, improvement of clinical symptoms of anxiety and depression, suggests that neurofeedback training also improves general well-being in this population.
References
- Moeller, F.G., et al., Increased impulsivity in cocaine dependent subjects independent of antisocial personality disorder and aggression. Drug Alcohol Depend, 2002. 68(1): p. 105-11.
- Ortal, S., et al., The Role of Different Aspects of Impulsivity as Independent Risk Factors for Substance Use Disorders in Patients with ADHD: A Review. Curr Drug Abuse Rev, 2015. 8(2): p. 119-33.
- Rodriguez-Cintas, L., et al., Impulsivity and addiction severity in cocaine and opioid dependent patients. Addict Behav, 2016. 58: p. 104-9.
- Roncero, C., et al., Cocaine-induced psychosis and impulsivity in cocaine-dependent patients. J Addict Dis, 2013. 32(3): p. 263-73.
- Valero, S., et al., Neuroticism and impulsivity: their hierarchical organization in the personality characterization of drug-dependent patients from a decision tree learning perspective. Compr Psychiatry, 2014. 55(5): p. 1227-33.
- Coffey, S.F., et al., Impulsivity and rapid discounting of delayed hypothetical rewards in cocaine-dependent individuals. Exp Clin Psychopharmacol, 2003. 11(1): p. 18-25.
- Poling, J., T.R. Kosten, and M. Sofuoglu, Treatment outcome predictors for cocaine dependence. Am J Drug Alcohol Abuse, 2007. 33(2): p. 191-206.
- Laudet, A.B., What does recovery mean to you? Lessons from the recovery experience for research and practice. J Subst Abuse Treat, 2007. 33(3): p. 243-56.
- Winhusen, T., et al., Impulsivity is associated with treatment non-completion in cocaine- and methamphetamine-dependent patients but differs in nature as a function of stimulant-dependence diagnosis. J Subst Abuse Treat, 2013. 44(5): p. 541-7.
- Barratt, E.S., et al., Neuropsychological and cognitive psychophysiological substrates of impulsive aggression. Biol Psychiatry, 1997. 41(10): p. 1045-61.
- Patton, J.H., M.S. Stanford, and E.S. Barratt, Factor structure of the Barratt impulsiveness scale. J Clin Psychol, 1995. 51(6): p. 768-74.
- Winstanley, C.A., D.M. Eagle, and T.W. Robbins, Behavioral models of impulsivity in relation to ADHD: translation between clinical and preclinical studies. Clin Psychol Rev, 2006. 26(4): p. 379-95.
- Winstanley, C.A., et al., Insight into the relationship between impulsivity and substance abuse from studies using animal models. Alcohol Clin Exp Res, 2010. 34(8): p. 1306-18.
- Chester, D.S., et al., How do negative emotions impair self-control? A neural model of negative urgency. Neuroimage, 2016. 132: p. 43-50.
- Kreibig, S.D., Autonomic nervous system activity in emotion: a review. Biol Psychol, 2010. 84(3): p. 394-421.
- Tanabe, J., et al., Medial orbitofrontal cortex gray matter is reduced in abstinent substance-dependent individuals. Biol Psychiatry, 2009. 65(2): p. 160-4.
- London, E.D., et al., Orbitofrontal cortex and human drug abuse: functional imaging. Cereb Cortex, 2000. 10(3): p. 334-42.
- Stapleton, J.M., et al., Cerebral glucose utilization in polysubstance abuse. Neuropsychopharmacology, 1995. 13(1): p. 21-31.
- Volkow, N.D. and J.S. Fowler, Addiction, a disease of compulsion and drive: involvement of the orbitofrontal cortex. Cereb Cortex, 2000. 10(3): p. 318-25.
- Volkow, N.D., et al., Long-term frontal brain metabolic changes in cocaine abusers. Synapse, 1992. 11(3): p. 184-90.
- Fingelkurts, A.A., et al., Increased local and decreased remote functional connectivity at EEG alpha and beta frequency bands in opioid-dependent patients. Psychopharmacology (Berl), 2006. 188(1): p. 42-52.
- Franken, I.H., et al., Electroencephalographic power and coherence analyses suggest altered brain function in abstinent male heroin-dependent patients. Neuropsychobiology, 2004. 49(2): p. 105-10.
- Prichep, L.S., et al., Quantitative electroencephalographic characteristics of crack cocaine dependence. Biol Psychiatry, 1996. 40(10): p. 986-93.
- Roemer, R.A., et al., Quantitative electroencephalographic analyses in cocaine-preferring polysubstance abusers during abstinence. Psychiatry Res, 1995. 58(3): p. 247-57.
- Hammond, D.C., Neurofeedback with anxiety and affective disorders. Child Adolesc Psychiatr Clin N Am, 2005. 14(1): p. 105-23, vii.
- Johnstone, J., J. Gunkelman, and J. Lunt, Clinical database development: characterization of EEG phenotypes. Clin EEG Neurosci, 2005. 36(2): p. 99-107.
- Scott, W.C., et al., Effects of an EEG biofeedback protocol on a mixed substance abusing population. Am J Drug Alcohol Abuse, 2005. 31(3): p. 455-69.
- Horrell, T., et al., Neurofeedback Effects on Evoked and Induced EEG Gamma Band Reactivity to Drug-related Cues in Cocaine Addiction. J Neurother, 2010. 14(3): p. 195-216.
- Corominas-Roso, M., et al., Benefits of EEG-Neurofeedback on the Modulation of Impulsivity in a Sample of Cocaine and Heroin Long-Term Abstinent Inmates: A Pilot Study. Int J Offender Ther Comp Criminol, 2020: p. 306624X20904704.
- Corominas, M., C. Roncero, and M. Casas, Corticotropin releasing factor and neuroplasticity in cocaine addiction. Life Sci, 2010. 86(1-2): p. 1-9.
- DiGirolamo, G.J., et al., Increased Depression and Anxiety Symptoms are Associated with More Breakdowns in Cognitive Control to Cocaine Cues in Veterans with Cocaine Use Disorder. J Dual Diagn, 2017. 13(4): p. 298-304.
- Hasin, D., et al., Effects of major depression on remission and relapse of substance dependence. Arch Gen Psychiatry, 2002. 59(4): p. 375-80.