Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder associated with genetic biochemical anomalies, with presence in the US estimated at around 9.5% in children between 4 and 17 years of age, with symptoms persisting into adulthood in 50% of cases [1].
As indicated in the Diagnostic and Statistical Manual of Mental Disorders (DSM) [2] published by the American Psychiatric Association, three ADHD subtypes can be distinguished on the basis of the behavioral symptoms presented:
1) Predominately inattention type
2) Predominately hyperactivity-impulsivity type
(3) Combined type
However, accumulating research suggests that this classification can be largely inaccurate or at least incomplete, as it is only based on clinical interviews and scores in psychiatric questionnaires, not taking into account objective and reliable measures.
One diagnostic approach that, over the last two decades, has been gaining growing support from peer-reviewed research is based on the use of electroencephalography (EEG) to measure selective activation anomalies in the brain, as compared to a normative database gathered from healthy subjects.
The output of this comparison is called quantitative EEG (QEEG), which is used by the trained neurotherapist to make considerations that may complement and extend a diagnosis based only on behavioral symptoms [3].
For example, QEEG studies have shown that ADHD children with the combined type have activity deficit in the frequencies delta, theta, and alpha [4] (Fig.1 A), which are thought to be associated with hyperactivity and impulsivity. Also, in the combined type, the number of neurons activated at specific frequencies (a measure called coherence) across the two brain hemispheres has been shown to be greater than in the inattentive type [4] (Fig.1 B).

The information gathered by QEEG can then assist the therapist in choosing the intervention strategy that she/he deems most appropriate for the client, which may include talk therapy, pharmacotherapy, and/or other types of interventions aimed at more directly influencing brain activity (e.g., neurofeedback training).
QEEG is also employed to predict and evaluate the treatment effects of pharmacotherapy. For example, QEEG, combined with clinical interviews, can help the neurotherapist to monitor changes in brain activity as a response to the administration of methylphenidate [5] and even to identify the children who are more likely to respond to the medication [6].
QEEG is also regularly used to monitor the effects of neurofeedback training in ADHD and to personalize neurofeedback protocols for improved effects [e.g., 7, 8]. By viewing the activity pattern (brain map), for separate frequency bands, the therapist can decide which avenue to take in order to “normalize” an abnormal pattern.
For example, if a child with ADHD has inattention problems, his QEEG will very likely reveal abnormalities in his “attention network”. The neurotherapist can then tailor a neurofeedback treatment protocol to alleviate or cancel the disruption within the attention network.
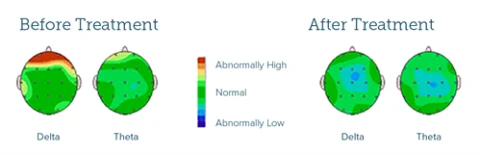
Also, a careful examination of the QEEG brain maps can help the therapist design a protocol to improve the functional connectivity between the attention network and other networks, if this is deemed necessary to produce optimal brain functioning. Fig.2 shows an example of a QEEG brain map before and after neurofeedback treatment of a child with ADHD.
Conclusions
The use of QEEG offers key advantages in the diagnosis of ADHD, allowing for greater objectivity and reliability in the identification of the disorder subtypes. QEEG also increases the objectivity and reliability in the evaluation of treatment response in both the pharmacotherapy and neurotherapy of ADHD.
References
- Berger, I., Diagnosis of attention deficit hyperactivity disorder: much ado about something. Isr Med Assoc J, 2011. 13(9): p. 571-4.
- Association, A.P., Diagnostic and Statistical Manual of Mental Disorders. 5th ed. ed. 2013, Washington, DC: American Psychiatric Association
- Galiana-Simal, A., et al., [Quantitative electroencephalography as a tool for the diagnosis and follow-up of patients with attention-deficit/hyperactivity disorder]. Rev Neurol, 2020. 70(6): p. 197-205.
- Rodrak, S. and Y. Wongsawat, EEG brain mapping and brain connectivity index for subtypes classification of attention deficit hyperactivity disorder children during the eye-opened period. Conf Proc IEEE Eng Med Biol Soc, 2013. 2013: p. 7400-3.
- Valdizan, J.R., [The diagnostic evaluation and therapeutic basis of immediate release methylphenidate in attention deficit hyperactivity disorder]. Rev Neurol, 2004. 38(6): p. 501-6.
- Sari Gokten, E., et al., Predictive Value of Slow and Fast EEG Oscillations for Methylphenidate Response in ADHD. Clin EEG Neurosci, 2019. 50(5): p. 332-338.
- Arns, M., W. Drinkenburg, and J. Leon Kenemans, The effects of QEEG-informed neurofeedback in ADHD: an open-label pilot study. Appl Psychophysiol Biofeedback, 2012. 37(3): p. 171-80.
- Arns, M., et al., Efficacy of neurofeedback treatment in ADHD: the effects on inattention, impulsivity and hyperactivity: a meta-analysis. Clin EEG Neurosci, 2009. 40(3): p. 180-9.